C-Desk Technology
01636 816466


Care Plan Templates
Available to download from Amazon Kindle
We ran a 54-bed Nursing Home and developed Care Plans as word processor
documents so everyone can use them, as well as software to run the staffing
scheduling.
Please note: you will definitely want to change these forms to your requirements
so they are easy to change. Word forms typically are very time consuming to
start from scratch, these give you that head start. They also give you a head
start in deciding what to put on the forms.
You can download each page individually from each of the Kindle ebooks.
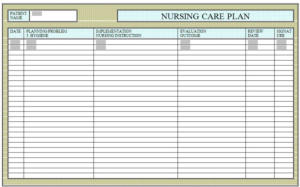
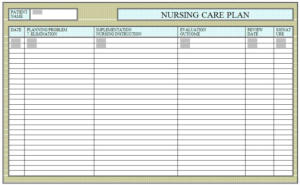
Care Plans & The Nursing Process -
This is a 5 step process nurses use to help look after their patients. It's
steps are very similar to the steps of the scientific process. It is usually
a systematic, rational method of planning and providing nursing care.
1 - Assessing - collecting, verifying and organizing data about the
patient.; data is obtained from reports, the patient.s chart and
measurements, your assessment, observation, other healthcare
personnel, interviews, etc
2 - Diagnosing / Analyzing - forming your nursing diagnoses; a nursing
diagnosis is a statement of an actual or potential health problem
3 - Planning - formulate your "plan" to assist the patient involves
formulating goals/expected outcomes, setting priorities, and identifying
nursing interventions to help patients reach their goals
4 - Implementing / Intervention - put your Nursing Care Plan into action
5 - Evaluating - evaluate your interventions, reasses and analyze, etc
Tuition and examples in using Care Plans to look after patients is
available from CDT
CDT produce a set of Care Plans to look after patients. These are word
processor Document templates. As templates, they can be generated
time and again for all your existing and new patients. The templates
can be edited by you in your Home to suit your working practices. You
can change the wording and the layout. You can add new lines of
information. If the spaces to input information are too small, then
simply increase the size of the space. These templates work just like
any other word processor document so you can fully customise them.
Once you have the document templates on your computer, you can
print off as many copies as you like for your Home or hospital (we only
ask that you leave our copyright on each document).













Kindle ebooks
A Clothing Form was filled in at our Nursing
Home soon after admission. The quantity and
quality of clothing is an important factor in the
wellbeing of a patient. Items had to be suitable
for the patient and easy to put on and take off.
Everyone gets dressed every day
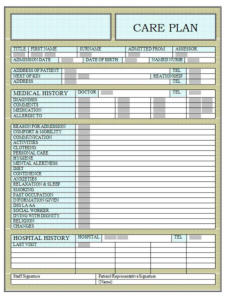
All our patients had a History Form.
The form was initially filled in by the
senior nurse on duty at the time of
admission. The form was filled in
with information from the patient
or with the help of the person
currently caring for them, be that a
carer, another Home or hospital, and
by observation. This enabled the Home
to prepare a full care plan of how they
would be cared for. The doctor, district
nurse or social worker could be
involved in this process.
The information on this form could be checked
against the Pre-Admission Assessment Form as
a check on any deterioration in the condition of
the patient as these forms may be filled in
weeks or even months apart.
It is at this point in the process that addition
information can start to be compiled and
added to the documents. This can include
a photograph of the patient, photographs a
ssociated with the condition of the patient,
contact details for associated services such
as optician, chiropodist, physiotherapist.
Each patient is assessed regarding admission
into the nursing home. This form details the
patients condition, health, level of support
required, previous medical condition, previous
hospital history and everything of interest
regarding an anticipated admission.
All the forms can be expanded as required
and new categories added for individuals.
The form was initially filled in by the
senior nurse on duty at the time of
admission.
The information on this form could be
checked against the Pre-Admission
Assessment Form as a check on any
deterioration in the condition of the
patient before and after admission.
The information on this form could be
checked against the Pre-Admission
Assessment Form as a check on any
deterioration in the condition of the
patient as these forms may be filled
in weeks or even months apart.
It is important to determine if the patient
already has diabetes or is exhibiting signs
of imminent diabetes.
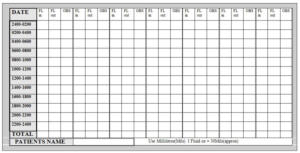
This form is to detail the fluid intake and
elimination of the patient in sufficient
detail that a diagnosis can be made and
the planning of the care process can begin.
What fluid was taken and how often.
A check on the urine is also needed, is it
normal, its colour, smell or blood. Notes
about the medication, special treatments
and diets, specialist equipment such as a
catheter and so on can be included.
It is important to determine if the patient
already has mobility problems.
You need to know how mobile your patient is,
fully mobile, wandering, wheelchair use, when
in bed is helping required with change of position.
When handling your patient, are they at risk from
shear or pressure changes.
This form is to detail whether there are any
communication problems. Do they have a
hearing aid or have had a stroke that
affects their speech.
Depending on the patient’s condition different
activities could be perused. Reading a book or
newspaper or having it read to them. Use of
talking books & local newspapers with
individuals or used in group discussion. Use of
music, or photographs to bring back pleasant
memories from the past to share with others.
A Hygiene form was filled in soon after admission.
Each patient was allocated their special nurse
whose job was to note any changes in the skin as
skincare took place. If redness or a break in the
skin was noted the pressure sore form was filled
in. Also skin infections, rashes, spots or boils,
surgery and healing, types of soap, etc.
A diet form was filled in soon after admission.
All patients were asked about problems,
dentures, swallowing, help required at meal times.
Our cook visited each patient so each could be
catered for individually.
A note was made about drinks and drinking.
An elimination form was filled in soon after
admission. This detailed whether there were
any continence problems or bowel problems.
Details about laxatives, or roughage was
required. Whether there were any smells or
color changes.
A rest and relaxation form was filled in soon after
admission. These are important factors in the
wellbeing of a patient. Factors such as noise,
lighting or other patients’ noises can result in
sleep deprivation. Problems associated with
sleep tend to be reported by night staff.
A dying with dignity form was filled in soon
after admission. This is checked with relatives
and friends and their contact details were
correct. Religious and cultural needs are
noted. Noted also are the Doctor, religious
presence, undertaker, and if relatives would
like to be present.
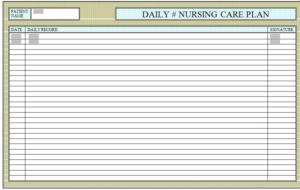
A daily record form was filled in at least once a
day, or more often as events happened. It is
important to know if ‘nothing happened’ as much
as if something happened so that you know
nothing is missing from the record.
A lifting and handling form was filled in soon after
admission. This enables a full care plan to be set up
for each patient. This includes setting up appro-
priate methods of lifting, having the right
equipment available and instructing the staff.
A health and safety form was filled in soon after
admission. This detailed the equipment required
regarding mobility, rest, sleep and their general
condition. Details such as cot sides and a bathing
hoist were recorded here.
The Kindle Books are
available in your country’s
store. Just do a search for
the author,
Kathleen Jezewska SRN








The aim of this book is to teach you
how to calculate how many staff you
need to run your operation.
The aim of this series of books is
to provide a reference guide for t
he types of available shift patterns
by way of supplying a total of
almost 300 unique shift patterns.
This book is about how to organise
staff holidays so that they do not
affect the operation. A Holidays
Included Shift Pattern will
accommodate everyone’s holiday
in the shift pattern.
This book looks at the details of
introducing and using Banked
Hours based on our experiences
with the many organisations
that use them.
This book not only includes easy to
follow examples of how to calculate
your Absence Rate, but also shows
you how to use your Absence Rate
to predict how absences will occur
in the future. This book has look-up
tables which convert Absence Rate
in to the number you would expect
to be off shift.
Shift working is also more fatiguing than
office hours working; this is especially
prevalent if working nights. However this
book is about minimising fatigue and the
effects of fatigue so that you can enjoy
the advantages of working shifts without
being too fatigued.
Managing holidays are the bane of all
managers. The aim of this book is to
show you some simple techniques to
relieve you of the burden. With a
special section on Office Hours, this
book is ideal for all managers.
Have you found that the year is just not
long enough to fit in all the holidays?
The aim of this book is to help
managers with their shift
operations. Holidays and absences
can play havoc with most operations
unless special procedures are in place.
This book provides the solutions used
by us when setting up a shift system.


C-Desk Technology | Old Vicarage | Rolleston | NG23 5SE | Tel: (+44) 01636 816466 | alec@visualrota.co.uk
Microsoft Word Forms
Setting up a form in Word is not easy and getting it to perform as you would want it is even harder. Our forms are designed to be flexible enough so you can alter them to suit your requirements. Word enables you to combine documents into one file, and in the file you can add scans, such as medical notes, or photographs and even videos. That way, the forms can be different for each patient as required. All their information is in one place on the computer but also accessible everywhere else.
Operational Efficiency
We created the forms so that everyone knew where they were
when required and by printing off the forms each day, they
could be with you if you worked away from a computer.
A nursing home or hospital is a very busy place with visits from
Doctors, physios, nurses, and many other professionals every
minute of the day. Having the information on the computer
and printed out meant you can send out a copy when a patient
went to the hospital, or show a relative, or review with the
Doctor in the office and accompany the Doctor doing their
rounds.
History Form

More pages
Management Scheduling Services Industries News Clients About Shop Contact
Reducing Costs &
Increasing Quality
1. Ensure all shifts are fully staffed 2. Ensure all shifts are fully skilled 3. Ensure everyone can take all their holiday 4. Call or email us
BLOGS
•
Holiday Entitlements,
•
Cover Shifts,
•
Easter,
•
Fair Holiday Scheduling,
•
High Sickness,
•
Forward Planning,
•
Skiing,
•
Frosty Mornings,
•
10-hour Shifts,
•
How Good is your Maths,
•
Unlimited Holidays,
•
Stagger Lunch,
•
Optimise Equipment,